


ORTHOLUTION
Next Generation of Orthodontic mini-implant
-
Loosening of the orthodontic implant
- Loosening of the orthodontic implant
- Fracture of the orthodontic implant
- Treatment of the fractured tip
- Injury of periodontal tissue
- Infection and abscess
- Damage of neighboring soft tissue
- Orthodontic implant covered with soft tissue
- Pain during implantation
- Pain during mastication
- Implantation in inappropriate area
Loosening of the orthodontic implant
Orthodontic treatment facilitated by orthodontic implant is becoming universal. However, problems from orthodontic implants are also increasing.
Loosening of the orthodontic implant
Although the success rate of ORLUS orthodontic mini-implants may have increased, loosening of the orthodontic implant may also occur; this situation is very embarrassing. Epidemiological studies have pointed towards the following: most failures arise from the bone-implant interface and most failures occur shortly after implantation. The failures of the bone-implant interface come from inadequate primary stability, excessive surgical trauma, and unfavorable healing conditions. During treatment, impact stress or irritation from surroundings may also cause loosening.
For using orthodontic implants that have an improved structure for enhanced stability, the use of a standardized procedure with full understanding of the mechanism can increase the rate of success (figure 1, 2). Additionally, the operator must also focus on the procedure.
The patient must be informed of the possibility of loosening of implants and the possibility of re-implantation before the surgical procedure. Pre-medication for pain control is very important, and is also effective in decreasing anxiety in the event that re-implantation is necessary after initial failure.
When a tight fit is not felt during the final stage of the insertion procedure, this indicates that sufficient primary stability can not be obtained and that the implant will probably fail. This is caused by poor bone quality, wobbling, or unintentional excessive surgical trauma during insertion. If this situation occurs, the following may be helpful; first, the presence of poor bone quality or poor primary stability should be noted to the patient or parents of the patient because the patient may be surprised at unexpected implant loss. Second, changes to orthodontic implants with wider diameter and deeper insertion should be considered. Third, additional insertion at another site should be considered. A NiTi coil spring with a light force of no more than 100 gm is also recommended. After confirmation of stability, orthodontic force may be increased.
If mobility of an implant is detected at the follow-up appointment, the implant should be considered as a failure. However, in case of slight mobility, the following form of management can be considered: deeper insertion under infiltration anesthesia will increase mechanical stabilization due to the unique design of the new type of implant. This procedure should only be performed after the patient or parents of the patient have been notified. Use of a NiTi coil spring is also recommended. It should be noted that when insertion is made deeper, the chance of burial by soft tissue increases.
The success rates in individuals younger than 15 years of age are relatively low because the bone quality and quantity is relatively poor in young teenage. Therefore, the protocols for younger patients should be followed(Vol.2 Site selection, p2).
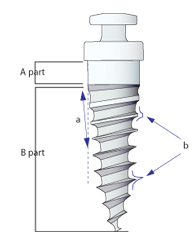
Fig. 1 Understanding of the design: the ORLUS mini-implant has a unique structure; it can be inserted to a greater depth, and more support can be obtained from cortical bone because it has a tapered core(a) that widens with height and a dual thread(b) which consists of trapezoidal threads in the cervical area and reverse buttress threads in the apical area. The A part area without threads is designed for contact with the soft tissue while the area B part area with trapezoidal threads is designed for contact with cortical bone to obtain primary stability. In every case, the B part area should remain in contact with cortical bone for stability. And for areas with thick soft tissue, the A part area of an implant should be of appropriate length for the thickness of the soft tissue.
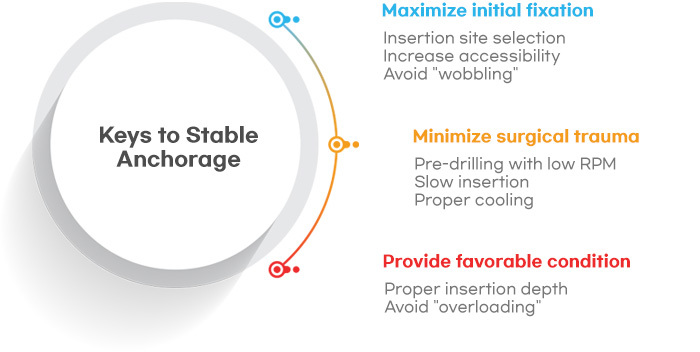
Fig. 2 Three key points for stable anchorag
- 상호 : (주)오솔루션
- 대표자 : 김정문
- 주소 : 서울 강동구 양재대로 1371 (성내동) 207호
- TEL : 02-483-1212
- FAX : 02-478-0735
- 사업자 등록번호 : 212-81-63456
- EMAIL : orlus@ortholution.com
- Copyright(c) (주)오솔루션. All Rights Reserved.

