


ORTHOLUTION
Next Generation of Orthodontic mini-implant
-
Selection of the insertion site
Selection of the insertion site
Selection of an insertion site in non-growing patients
Though the cortical bone of the maxilla is considered a thin bone in the body, it is thick enough to provide sufficient primary stability in orthodontic anchorage; thus, the buccal alveolus can be considered the best site for insertion because of its favorable accessibility. For cases in which higher biomechanical efficacy is required, such as molar intrusion, implantation on the palatal side (the posterior palatal alveolus or the midpalatal suture area) should be considered. The cortical bone of the mandible is thicker than that of the maxilla, and is thus advantageous for obtaining primary stability. However, possible irritation by food during mastication serves as a disadvantage. Furthermore, in the mandible, the lingual side is not feasible for the placement of an implant because the tongue is located in this area and this could lead to patient discomfort. The tongue may also compromise the overall accessibility. In most cases, the following three areas; the maxillary buccal alveolus, the posterior palatal alveolus, and mandibular buccal alveolus provide a reasonable number of insertion sites for orthodontic mini-implant anchorage.
| fail-safe | accessibility | discomfort | hard tissue | soft tissue | availability | irritation | total | |
|---|---|---|---|---|---|---|---|---|
| buccal alveolus |
A | A | A | B | A | A | cheek | A |
| edentulous area | A | A | A | B | A | A | . | A |
| post palatal alveolus | A | B | A | B | A | A | tongue | A |
| midpalatal suture | A | B | C | A | A | C | tongue | B |
| anterior alveolus | B | A | B | A | B | A | lip | B |
| anterior rugae area | A | B | B | A | A | A | tongue | B |
| infrazygomatic crest | B | A | C | A | C | A | tongue | C |
| Mx tuberosity area | B | C | A | B | A | A | . | C |
| fail-safe | accessibility | discomfort | hard tissue | soft tissue | availability | irritation | total | |
|---|---|---|---|---|---|---|---|---|
| buccal alveolus |
A | A | A | A | A | A | cheek | A |
| edentulous area | A | A | A | B | A | A | . | A |
| anterior alveolus | B | A | B | A | B | A | lip |
B |
| buccal shelf | A | B | C | A | C | A | cheek | B |
| retromolar area | C | C | B | A | B | A | muscle | B |
| lingual alveolus | A | C | C | A | A | A | tongue | C |
Selection of an insertion site in growing patients The following should be taken into consideration.
- In order to prevent injury to successor tooth buds, areas in which permanent teeth have not yet erupted should be avoided whenever possible.
- The bone quality and quantity is relatively poor in young teenage patients so as to be disadvantageous in obtaining primary stability (figure 1). The relatively low success rates in individuals younger than 15 years of age should be noted beforehand; in particular, the stability in the maxillary buccal area may be relatively low.
- Pre-drilling through cortical bone is recommended to minimize surgical trauma as much as possible.
- The area between the 1st and 2nd premolars provides more favorable accessibility as well as slightly superior bone quality. Thus, this area should be chosen over the area between the 2nd premolar and 1st molar.
- Implants should be inserted deeper to minimize stress from the oral environment during the healing and treatment periods.
- The use of light continuous force is preferable over the use of heavy intermittent force. In other words, NiTi coil springs should be used instead of elastomeric chains. The applied force should not exceed 150gm.
- In the case of repeated failure, the midpalatal suture area should be considered because the bone quality and quantity of the midpalatal suture is better than that of other areas. There is still sutural growth in the midpalatal suture of young patients, so the parasagittal area may be considered.
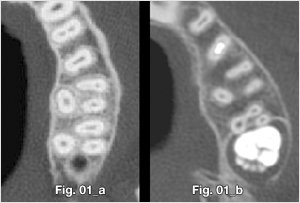
Fig. 1 When comparing the buccal cortical bone of adults (a) with that of patients younger than 15 years old (b), younger bone shows comparatively poor bone quality and quantity. Therefore, it is hard to obtain primary stability in younger patients.
- 상호 : (주)오솔루션
- 대표자 : 김정문
- 주소 : 서울 강동구 양재대로 1371 (성내동) 207호
- TEL : 02-483-1212
- FAX : 02-478-0735
- 사업자 등록번호 : 212-81-63456
- EMAIL : orlus@ortholution.com
- Copyright(c) (주)오솔루션. All Rights Reserved.

