


ORTHOLUTION
Next Generation of Orthodontic mini-implant
-
Precautions according to insertion site: Mandible
Precautions according to insertion site: Mandible
Mandibular buccal alveolus
In contrast to the maxilla, extra caution is necessary because the mandible houses the mandibular canal, an important anatomical structure (figure 38, 39). The risk of injury to the canal is quite low as long as the implant tip does not surpass the tooth apex, but the course of the canal must always be checked by panoramic radiography prior to an insertion procedure. The cortical bone of the mandible is thicker than that of the maxilla and provides better primary stability. However, in cases of thick and hard cortical bone, surgical trauma due to frictional heat or excessive pressure during implantation increases. The risk of implant fracture also increases, and poor accessibility makes matters worse. If contra-angled instruments are used for insertion, the risk of implant fracture is also increased by the leverage effect. The excessively large insertion torque indicates that strong pressure is delivered to the adjacent bone structure, and this means that the risk of implant fracture is also drastically increased. And it may also be the sign of overstress to adjacent bone tissue, so reverse rotation should be performed to relieve stress on adjacent bone during the guiding stage. But, reverse rotation should never be used during the finishing stage.
Additional irritation by food during mastication may compromise stability. Stability may especially be decreased in the areas between the mandibular 1st and 2nd molars because of irritation from food during mastication and pressure from the cheek muscles. Centric occlusion in the molar area must be checked; if possible, the implant should be placed at a point where the stress from mastication can be minimized.
Besides this, implantation in the mandibular alveolus is quite similar to that in the maxillary buccal area.
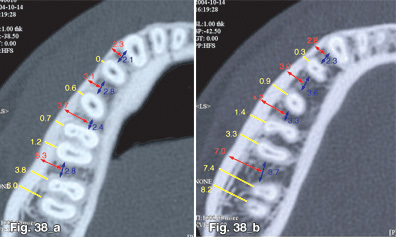
Fig. 38 The distance between the mandibular teeth at 4mm (a) and 8mm (b) apical from the CEJ. As was the case in the maxilla, the available buccolingual space is quite narrow in the anterior area and the premolar area.
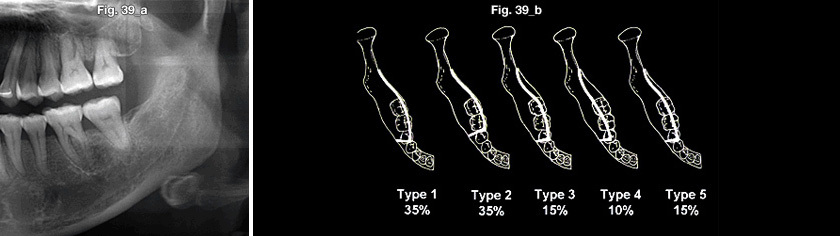
Fig. 39 The pathway of the mandibular canal can be observed on the panoramic radiograph. From the buccolingual dimension, it is generally located to the lingual side (b). However, there is little possibility that the canal will be damaged unless implants are inserted below the level of the root apex.
Implant selection
Implantation is similar to that in the maxillary buccal area. However, special care should be given in harder bone to prevent implant fracture and to minimize surgical trauma. In most cases, a regular type of implant is chosen, but a wide type may be used in growing patients or when sufficient primary stability is not indicated during the implantation of a regular type.
Determination of insertion site and angle
Determination of insertion site and angle is similar to that in the maxilla (figure 40). However, when placing the implant between the mandibular 1st and 2nd molars, the occlusion and vestibular space should be checked. The implant position should be determined with the consideration of possible stress from mastication and from the buccinator muscle.
Implantation angle: Oblique implantation may allow the use of more buccal and interdental space, and may also reduce the possibility of root injury while increasing the contact area with cortical bone. However, depending on the buccal slope of the cortical bone, oblique implantation may be impossible (figure 41), as in the maxilla.
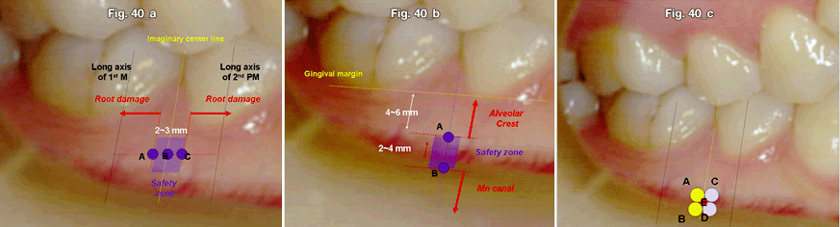
Fig. 40 Determination of the insertion site is similar to that in the maxilla.
- For molar distalization, an insertion position 1.5mm distal to an imaginary central line between two teeth should be determined. For molar protraction, an insertion position 1.5mm mesial to an imaginary central line should be determined. If there is to be no mesio-distal movement of adjacent teeth, an insertion position on the central line should be determined.
- For intrusion, an insertion position should be determined of sufficent depth apically. Otherwise, implants will restrict further intrusion.
- The insertion position should be determined according to the antero-posterior and vertical tooth movement required.
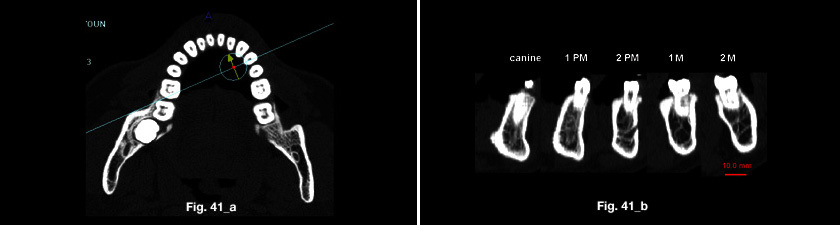
Fig. 41 Like the maxillary buccal side, the surface topography of cortical bone is different according to the area and within each individual. When taking a look at the buccolingual section (a), the closer to the anterior teeth, the more inclined the implant is to the labial side (b). Hence, the working angle during insertion should be determined according to the surface topography of the cortical bone, as it was for the maxilla.
Retromolar area
The implant is advantageous for the distalizing force and single force for molar uprighting to be delivered, and it can produce an extrusive force vector with distalization (figure 42). Additionally, this implant does not interfere with tooth movement. However, the mandibular canal is close to the retromolar area, and many important anatomical structures that require special attention during implantation are present in this area as well (figure 43). Although the possibility of injuring the mandibular canal may be low, if injured, the outcome can be disastrous. Before implantation, the passage of the mandibular canal should be assessed through panoramic views and the bone bed should be ensured through palpation (figure 44). During implantation, even if little doubt exists, a periapical radiograph should be taken and safety should be reassessed.
This site is easily covered because it is an area in which soft tissue is thick and movable, though this may differ in individual patients. The tissue condition of the retromolar area varies in individuals. For example, in cases with a developing 3rd molar tooth bud, insufficient space on the distal side of the molar or narrow interocclusal space may restrict implantation. Opposing teeth or the maxillary tuberosity can restrict the vertical space, so the opposing relation of the usable space should be assessed in advance. Since soft tissue is thick and very mobile, maintenance is difficult and may render the open method difficult.
One other disadvantage is the excessively hard condition of the bone. Hard and rich cortical bone can provide good primary stability, but it may also increase the surgical trauma and the risk of implant fracture. It is mandatory that pre-drilling be performed through the cortical bone at all times in the retromolar area. Because of the shape of the mandible itself, caution should be taken to prevent injury to the inner side of the ramus and the canal.
Due to these factors, special consideration should be taken for implantation. Pre-surgical examination and a proper mechanic treatment plan are of the utmost importance. The thickness and mobility of soft tissue and the relationship with opposing maxillary teeth should be assessed before implantation. Flap surgery is helpful to increase visibility and accessibility to prevent iatrogenic injury. If surgical removal of an impacted 3rd molar is planned, it is preferable that extraction and implantation be performed together. Pre-drilling through cortical bone with palpation of the implantation site should always be performed in advance to confirm the position of the bone bed. Pre-drilling can reduce surgical trauma and the risk of implant fracture.
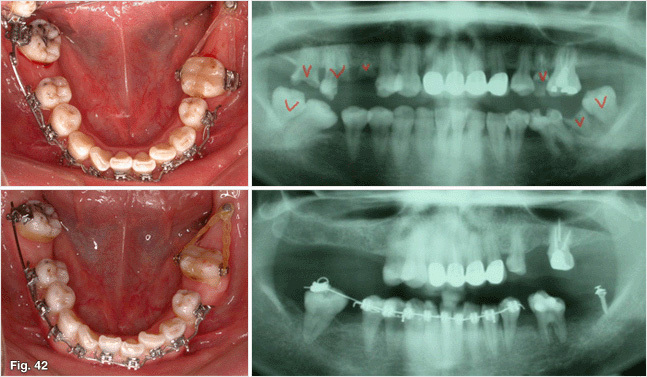
Fig. 42 When the posterior teeth are lost, there is the sufficient space for the implant insertion at the retromolar area. The mesially angulated molar was uprighted using the single force from the mini-implant.

Fig. 43 A lot of important anatomical structures are present in the retromolar area, especially on the inner side of the ramus. The lingual nerve travels near the retromolar area and the mandibular canal is also close to the retromolar area. Therefore, much attention is needed to prevent injury to significant structures.

Fig. 44 The mandible appears to be a shape much like a combination of the letters U and V, so the retromolar area exists in a lateral site to the most posterior molar. Before inserting an implant in the retromolar area, the bone bed should be confirmed through palpation as not to insert into the soft tissue.
Selection of implant
First, before insertion, the insertion site should be examined by assessing the soft tissue condition using a periodontal probe and determining the thickness of soft tissue. The available vertical space with opposing teeth or maxillary tuberosity should also be assessed. Then, whether the open method or the closed method will be used should be determined according to the soft tissue condition and available vertical space. In order to use an open method, the implant head should be sufficiently exposed. For cases with insufficient interocclusal space or thick and movable soft tissue, a closed technique may be considered.
Buccal shelf
Precautions are needed to prevent injury to the teeth and the mandibular canals.
Its advantages include thick cortical bone and abundant mesio-distal space, which does not restrict tooth movement. Additionally, it is in a good position to deliver intrusive forces, distalizing forces, and expansion forces to correct scissor bites (figure 45).
However, being in the vestibule area with excessive soft tissue movement, the cheek muscles can irritate the implant, which may lead to loosening and maintenance problems
Since cortical bone of this area is very hard, pre-drilling is necessary.
Implantation should be placed a certain distance from the vestibular fornix (mucobuccal fold). The implant head should never be placed more buccally across the vestibular fornix (the muccobuccal fold) (figure 46).
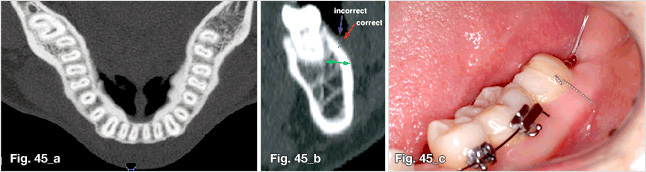
Fig. 45 Biomechanically, this is a good place to apply a single force for correction of the second molar scissor bite. There is sufficient space in the buccal side of the second molar (a,b), so a scissor bite can be corrected using a closed technique (c). During the procedure, it is important to insert with the proper direction and angle so as not to damage roots (b).
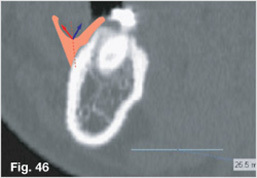
Fig. 46 An implant head or an extension wire should not be located lateral to the mucobuccal fold because of the excessive stress from facial muscles, such as the cheeks. The implant should be positioned medial to the mucobuccal fold.
Implant selection
An implant is selected according to the tissue conditions of the implantation site and the desired application method. For an open method to expose the head of the implant, one with soft tissue contact of more than 2mm may occasionally be needed, but when there seems to be a great chance of irritation from the cheek muscle, the closed method is preferable, especially for correction of a scissor bite.
Anterior alveolus
The bone quality of the anterior alveolus is superior, and this is an ideal position at which to provide the intrusive force to the anterior teeth (figure 47, 48). However, available space is limited because of the narrow labiolingual dimensions and interdental space. Continuous irritation from lip muscles may cause a problem.
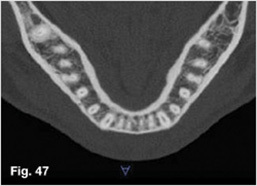
Fig. 47 The mini type is recommended for anterior alveolus because of the narrowness of the available space. The available bucco-lingual space of the anterior teeth is less than that of the molars. Furthermore, the interdental space of the mandibular anterior teeth is much narrower than that of the maxillary anterior teeth.

Fig. 48 Frena in the maxilla and mandible near the insertion sites called for frenectomies to be performed with the insertions so that the implants could be used by the open method without any further problems.
- Before insertion
- 1-week after the frenectomy and insertion
Edentulous area
The edentulous area is available for implant insertion but bone resorption as well as poor compact bone quality may be present and as a result, there may be a higher chance of improper primary stability.
Lingual alveolus
It is a good position in which to provide intrusive lingual forces, as well as constriction forces for posterior teeth. Thin soft tissue and good cortical bone provide adequate primary stability, but poor accessibility and continuous tongue irritation may compromise this stability. Most of all, the greatest disadvantage is the patient discomfort caused by the tongue. There are important anatomical structures present in the floor of the mouth; thus, implantation should not be placed too inferiorly beneath the floor of the mouth.
- 상호 : (주)오솔루션
- 대표자 : 김정문
- 주소 : 서울 강동구 양재대로 1371 (성내동) 207호
- TEL : 02-483-1212
- FAX : 02-478-0735
- 사업자 등록번호 : 212-81-63456
- EMAIL : orlus@ortholution.com
- Copyright(c) (주)오솔루션. All Rights Reserved.

