


ORTHOLUTION
Next Generation of Orthodontic mini-implant
-
Principles for surgical procedure of the new type of mini-implant
Principles for surgical procedure of the new type of mini-implant
Surgical principles Surgical procedures should be based on the following basic principles:
- Aseptic principle
- Atraumatic procedure
- Proper pre-operative exam & precise positioning
- Standardization
- Pre-medication for pain control
Aseptic principle
Implants and instruments should be used under aseptic conditions. The driver tip is a female type, so blood and saliva can gather easily in the driver tip. The driver tip should be cleaned with a smooth brush and a neutral detergent as soon as possible following the conclusion of the procedure.
Recycling of implants is prohibited by law and is also unfavorable from the viewpoint of stability because the surfaces of implants are treated in order to increase biocompatibility and when in contact with body fluid, the surface changes continuously from the initial state. If there is even a small amount of surface contamination, the implant can be used after cleaning with an ultrasonic cleaner and autoclaving. But repeated autoclaving also has adverse effects on the biocompatibility of the surface.
Atraumatic procedure
Bone healing process proceeds very slowly. Therefore, it is essential to minimize surgical trauma during implant placement as much as possible in order for favorable healing to occur. To minimize surgical trauma, the following issues should be kept in mind.
The drilling procedure should be performed with the use of well-sharpened drills under flowing saline cooling. Appropriate cooling is needed to minimize damage due to the heat generated during the insertion procedure.
If insertional torque seems to increase abruptly, further insertion is undesirable because this may be a sign of overstress to adjacent bone tissue. Thus, reverse rotation should be used to relieve stress on the adjacent bone. However, reverse rotation should never be used during insertion of the last 2mm of an implant, otherwise sufficient primary stability cannot be obtained.
Pre-op exam & proper positioning
Unnecessary injuries to the anatomical structures should be minimized based on full awareness of the anatomy of the insertion area. More specifically, if the movement of teeth adjacent to an implant is planned, precise positioning of implants should be preceded to secure enough available space.
Pre-medication for pain control
Pain control is very important to secure patient compliance. In the case of loosening, re-insertion is necessary, but experience of the first surgical placement of implants can greatly influence compliance of the second placement. For efficient pain control, pre-medication with analgesics(Acetaminophen 500mg) one hour prior to or at surgery and analgesics(Acetaminophen 500mg) three hours after at surgery are recommended for pain control. In general, preventive systemic antibiotics or systemic antibiotics after surgery are not necessary.
Standardization
Although the ORLUS mini-implant has a structure to minimize the influence of the operators dexterity, the condition of the operator may still influence the success rate. In other words, an improper and inaccurate procedure causes failure and stability can be improved by standardization and increased accessibility.
As noted previously, a surgical procedure should be performed based upon full understanding of the rationale of the design of the mini-implant, the biological mechanism, and the surgical principles.
In order for standardization, the surgical procedure is divided into 5 major stages, and specific goals should be achieved at each stage of the procedure before proceeding to the next stage. The five respective stages are: pre-op exam, marking, perforating, guiding, and finishing.
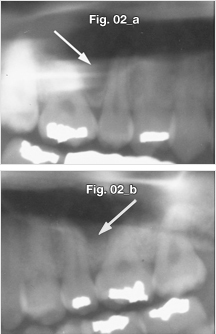
- Pre-op exam stage: site selection, anesthesia, and pre-op exam.(figure 2).
- Marking stage: marking the insertion position on the gingiva and soft tissue preparation.
- Perforating stage: perforating through cortical bone.
- Guiding stage: bone grip and determination of implantation angle.
- Finishing stage: finishing and obtaining mechanical stabilization from cortical bone.
Fig. 2
Pneumonization of the maxillary sinus may occur irrespective of age and presence of teeth, so the shape of the sinus should be checked by panoramic radiography.
Protocols for prevention of root injuries
Root injuries are rare, but very fatal. Therefore, protocols for prevention of root injuries cannot be overemphasized. In summary, pre-operative examination/marking on the gingiva, using the ORLUS Surgical drill (OS DRL-H116, OS DRL-E161, OS DRL-E162), pre-drilling through cortical bone and oblique insertion can all help to prevent root injuries. The ORLUS Surgical drill (OS DRL-H116, OS DRL-E161, OS DRL-E162) is 4.0mm long, so it can perforate cortical bone, but can only drill to a limited depth and cannot touch the root at the mucogingival junction. Pre-drilling through cortical bone makes the preceding insertion process easier by making insertion of the implant with minimal vertical force possible and increasing tactile sense during the procedure.
The use of only a small amount of vertical force is ample for insertion because cortical bone is perforated and cancellous bone shows little resistance to insertion. Be cautious not to exert a vertical force, particularly in the indirect approach, because tactile sense may be compromised. With a limited vertical force and an oblique angulation, the mini-implant cannot perforate or split the root.
If further advancement is limited during insertion, this will normally indicate root-touching.
- 상호 : (주)오솔루션
- 대표자 : 김정문
- 주소 : 서울 강동구 양재대로 1371 (성내동) 207호
- TEL : 02-483-1212
- FAX : 02-478-0735
- 사업자 등록번호 : 212-81-63456
- EMAIL : orlus@ortholution.com
- Copyright(c) (주)오솔루션. All Rights Reserved.

